

Healthy Skepticism International News
April 2008
Brief to Canada’s House of Commons Standing Committee on Postmarketing Surveillance of…
Brief to Canada’s House of Commons Standing Committee on Postmarketing Surveillance of Prescription Drugs
Executive summary
Drug safety is a serious issue and is increasing in prominence. In Canada 3-4% of drugs approved will eventually be withdrawn from the market because of safety issues but the numbers of people exposed to these drugs is increasing because of aggressive marketing tactics by the pharmaceutical industry.
The priorities of Health Canada are skewed in favour of rapid approval of new drugs at the expense of the postmarketing pharmacosurveillance system as judged by how money and personnel are allocated.
Faster approval of new drugs has the potential to produce more safety problems once drugs are on the market especially since Health Canada faces financial penalties if it exceeds targets for the length of time taken to approve products.
Although Health Canada has committed itself to achieving standards with regard to drug approval times, it has explicitly rejected developing quantitative standards for evaluating how its postmarketing pharmacosurveillance system. In addition to lacking standards in this area it has not made clear what its criteria are in issuing risk communication documents and it does not monitor whether or not those communications have had the desired effect in terms of changing the way that drugs are prescribed and used.
Adverse drug reactions (ADRs), even serious ones, are significantly under-reported but mandatory reporting does not seem to improve reporting rates in countries where it has been implemented. The United Kingdom uses a black triangle system to identify new drugs to remind doctors to report ADRs. New Zealand has the highest rate of reporting of ADRs in the world due to a variety of methods including the feedback that it provides to individuals filing reports and outreach strategies to emphasize the importance of reporting ADRs.
Canada’s postmarketing pharmacosurveillance system could be significantly improved through a series of reforms undertaken by Health Canada including:
•Health Canada needs to reorient its priorities so that postmarketing pharmacosurveillance is on an equal footing with approval of new drugs.
•Health Canada needs to devote significantly more resources to its postmarketing pharmacosurveillance system.
•Health Canada should undertake a systematic study to examine whether faster drug approvals lead to more postmarketing safety issues.
•Health Canada needs to develop measurable standards to judge its postmarketing pharmacosurveillance system.
•Health Canada needs to publicly and transparently explain what criteria it uses in issuing safety communications.
•Health Canada needs to systematically analyze whether its methods of communicating with health care professionals and the public are producing the desirable effects.
•Health Canada should adopt a form of the UK black triangle system to improve ADR reporting. One possibility is that a similar symbol could appear in the Compendium of Pharmaceuticals and •Specialties and on all promotional material. In addition, it could be made mandatory for drug company sales representatives to inform doctors about drugs carrying this symbol that are made by their company.
•Health Canada should study the methods that New Zealand uses in its postmarketing ADR system and adapt them for Canadian use.
Introduction
Drug safety is a serious issue that needs to be approached in a systematic manner. In the United States (US) Adverse Drug Reactions (ADRs) are between the 4th and 6th leading cause of death, contributing to more than 100,000 deaths and 1.5 million hospitalizations yearly.[1] Since that estimate was made in the late 1990s the severity of the problem has only heightened with a marked increase in reported deaths and serious injuries associated with drug therapy.[2] Although these figures come from the US there is no reason to believe that the situation is any different in Canada.
Over the past two decades about 3 to 4 percent of the drugs approved by Health Canada
subsequently need to be withdrawn from the market due to safety reasons (see Figure 1).
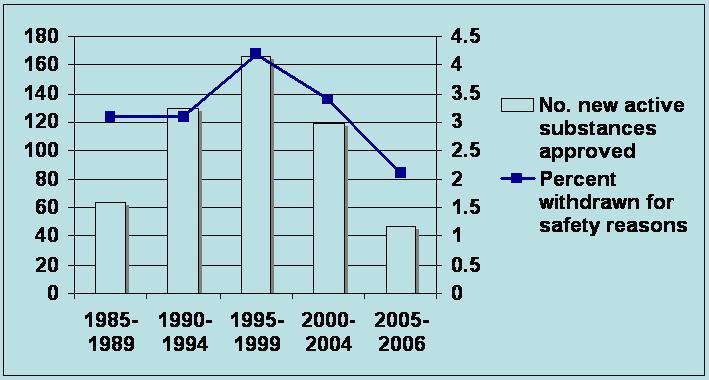
Figure 1: Safety withdrawals as a percent of approvals 1985 – 2006
Although the percentage of withdrawals has remained relatively stable, aggressive marketing of new drugs by drug companies means that an increasing number of people are exposed to these drugs before they are removed from the market. In the 2 – 4 years that bromfenac, dexfenfluramine and mibefradil were on the US market in the mid to late 1990s 6.4 million people were exposed to them.[3] Two of the 5 most heavily promoted drugs in Canada in 2000 (Baycol and Vioxx) were subsequently withdrawn because of safety issues. Furthermore, Table 1 shows that even drugs that have been on the market for a considerable length of time cannot be regarded as safe. Sometimes safety issues are not recognized for decades.
Table 1: Drugs withdrawn from the Canadian market since 2004
Health Canada’s priorities
Over the past decade, financing for the Therapeutic Products Directorate (TPD), the arm of Health Canada charged with approving new prescription drugs, has shifted from coming entirely from government appropriations to at one point drug companies providing 70% of funding and now about 1/3 coming from that source.[4] This shift in financing of the regulatory body has raised concerns about whether the TPD’s primary commitment is still to public health.
The apparent reorientation of the TPD in favour of business interests is further reflected in its Business Transformation Strategy (BTS) that is being implemented. The BTS was introduced in early 2003 and ‘builds on the commitments made by the Government of Canada to “speed up the regulatory process for drug approvals”, to move forward with a smart regulations strategy to accelerate reforms in key areas to promote health and sustainability, to contribute to innovation and economic growth, and to reduce the administrative burden on business’.[5]
One of the key phrases in the BTS is ‘smart regulation.’ Smart regulation means that Canada should ‘regulate in a way that enhances the climate for investment and trust in the markets’ and ‘accelerate reforms in key areas to promote health and sustainability, to contribute to innovation and economic growth, and to reduce the administrative burden on business’.[6] While health is not ignored, the emphasis is clearly on creating a business friendly environment. The federal External Advisory Committee on Smart Regulation explicitly states that risk management has an essential role in building public trust and business confidence in the Canadian market and regulatory system.[7]
When applied to drug regulation, risk management would mean weighing potential negative effects weighed against potential advantages. Potential negative effects would be adverse health effects that could occur under reasonably foreseeable conditions.[8] The shift from the precautionary principle to risk management is subtle but unmistakable. The precautionary principle says that if products cannot be shown to be safe then they should not be marketed; risk management allows products on the market unless they are shown to be harmful. Realigning regulation to conform to the principles of Smart Regulation would not totally abandon the concept of precaution but it seems to imply that there would have to be a threat of serious or irreversible damage before it would come into play.
The TPD is devoting significant organizational resources towards the goal of further speeding up the drug approval process. In the budget speech outlining government spending for the 2003 session of the federal parliament $190 million was allocated over a five year period mostly to improving ‘the timeliness of Health Canada’s regulatory processes with respect to human drugs’.[9] Forty million out of the $190 million was allocated for fiscal 2003-04. Out of that amount 78% ($31.2 million) is going toward ‘improved regulatory performance’ mainly an effort to eliminate the backlog in drug approvals and to ensure timeliness in getting drugs onto the market.[10] (Table 2)
Table 2: Allocation of $40 million dollars for improvements in drug regulatory system, fiscal 2003-2004
| Program area | Percent of money | Dollars ($ 000,000) |
| Improved regulatory performance | 78 | 31.2 |
| Enhanced post-marketing safety | 6.5 | 2.6 |
| Optimal drug therapy | 6 | 2.4 |
| Price review capacity | 1.25 | 0.5 |
| Therapeutic access strategy | 8.25 | 3.3 |
Source: Health Canada. (2003). Improving Canada’s regulatory process for therapeutic products: building the action plan. Ottawa: Public Policy Forum multi-stakeholder consultation.
This allocation of funding was made despite the fact that the TPD was already much more heavily resourced than the Marketed Health Products Directorate (MHPD), the
branch of Health Canada responsible for drug safety (Table 3) and as a result the MHPD had to stop routinely trying to assign causality when evaluating adverse drug reaction reports. Information from each adverse drug reaction report that is received is entered into a number of fields in the Canada Adverse Drug Reaction Information System (CADRIS) database. Because of increased workload and funding constraints, the number of essential fields in the CADRIS database has been reduced, such that the ‘causality’ field is no longer being systematically used.
Table 3: Relative funding of TPD and MHPD, 2004
| Directorate | Approximate annual operating cost base (year ended March 31, 2004) | Approximate number of employees (as at March 31, 2004) |
| Therapeutic Products Directorate | $38 million | 423 |
| Biologics and Genetic Therapies Directorate | $22 million | 228 |
| Health Products and Food Branch Inspectorate | $16 million | 190 |
| Marketed Health Products Directorate | $8 million | 90 |
| Total | $84 million | 931 |
Source: Progestic International Inc. Final report for the financial models project. Health Canada, May 2004.
Faster drug approvals and drug safety
Health Canada has committed to a maximum of 300 days for nonpriority drugs (180 days for priority drugs) and has devoted substantial resources to achieving this goal. Whether or not faster drug approvals result in a greater percentage of unsafe drugs reaching the market is the subject of an ongoing debate. Abraham compared drug withdrawals in the UK and the US in the period 1971-1992 (before the introduction of user fees in the US) and reported a ratio of 2.67:1 (24:9 drugs). His explanation for the lower number of withdrawals in the US was that the longer period spent examining the data in that country allowed regulators there to detect serious safety problems before products were marketed.[11] Estimates suggest that during the period 1990 to 1995 for every one month reduction in a drug’s review time there was a 1% increase in expected reports of adverse drug reaction (ADR) hospitalizations and a 2% increase in expected reports of ADR deaths.[12]
Carpenter and colleagues[13] suggest that the true effect of faster approvals on safety is not the overall rate of withdrawals but what happens to those drugs approved on the cusp of the approval deadline clock. (The FDA has a statutory requirement to approve 90% of new drug applications within specific periods of time depending on whether it is a standard or priority review. If it fails to meet that obligation then renewal of PDUFA may be endangered.) Their conclusion was that when drugs are approved in the immediate pre-deadline period there is a substantially higher rate of withdrawals and/or safety labeling changes compared to drugs approved after the deadline. In-other-words, it appears that if the deadline is imminent the FDA does a less thorough job of reviewing drugs in order to avoid crossing the deadline.
Similarly, revenue to the TPD will also suffer if service standards (approval of new drugs within the targeted time) are not met. If the actual performance in a given fiscal year is more than 110% of the target for that fee category, penalties apply for the amount in excess. Fees are then to be reduced for the next reporting year by a percentage equivalent to the performance not achieved, up to a maximum of 50%.[14] Faced with the prospect of penalties it is possible that the TPD might follow the pattern set by the FDA and approve new drugs to avoid incurring a financial loss in the next year.
Lack of measurable standards and absence of data for drug safety
As I have previously noted Health Canada, through its cost recovery initiative, has committed itself to achieving measurable standards with regard to drug approval times. However, it has no standards for safety issues. As one example there is no standard for the length of time that it will take between the receipt of an ADR and when that ADR has been analyzed and posted on Health Canada’s Medeffect Adverse Reaction Database. The United Kingdom commits to 3-7 days to process ADR reports and Australia targets initial professional review of adverse drug reaction reports within 3 days. Health Canada has explicitly rejected developing standards claiming that “development of quantitative service standards for post-market surveillance activities or compliance and enforcement activities is difficult given the unpredictability and volatility of the activities involved.”[15]
Although Health Canada has recently issued a draft guidance document about triggers for issuance of risk communication documents (available at: http://dsp psd.pwgsc.gc.ca/collection 2007/hc-sc/H164-48-2007E.pdf) it is unclear what methodology and information it uses in making its decisions. When important safety problems are identified with drugs the company manufacturing the product sends out a notice of the safety issue on behalf of Health Canada to health care providers and Health Canada posts a notice for the public on its web site. Single letters or web site announcements about safety problems have been shown to have little or no impact on prescribing of drugs.[16, 17] Health Canada does not make any efforts to monitor the impact of the safety information it provides or authorizes.
Reporting of ADRs
Passive ADR reporting systems world-wide are generally considered to capture only 1-10 percent of all reactions and that figure may in fact be considerably lower.[18] One French study estimated that even for serious and unlabelled reactions the estimated reporting rate was 1 in 4600.[19]
Would a mandatory system of reporting improve this situation? Almost half of Canadian doctors oppose mandatory reporting and view the requirement to report as an extra burden on their already busy lives.[20] Making reporting easier may help alleviate some of these concerns but Health Canada has not identified any concrete measures to do so. Payment to doctors for reporting is one option that has been suggested but currently more reports come from pharmacists than from doctors. Should pharmacists also be paid? Consumers/patients file about two thirds the number of reports that doctors do; if doctors and pharmacists are paid for reporting consumers and patients should also be compensated. Perhaps consumers should be paid more than health care professionals since reporting should be seen as part of their professional duty while consumers are under no such obligation.
Sometimes the analogy is made between reporting ADRs and child abuse but the two are not analogous. Any degree of child abuse is potentially serious and must be reported but the same is not true of all ADRs. An asymptomatic rash related to an antibiotic that will go away in a few days is clearly different from a cardiac arrhythmia that is life threatening. The former need not be reported while the latter must be.
Finally, reporting rates seem to be roughly the same in countries with mandatory reporting as in countries without.[21]
There are ways of improving ADR reporting. In the UK newly marketed drugs are marked with a black triangle, indicating that doctors should report all adverse reactions associated with these products to the Committee on Safety of Medicines. These black triangles appear beside the drug name in the British National Formulary and in promotional material.
New Zealand has the highest reporting rate of ADRs of all member countries in the World Health Organization International Drug Monitoring program both in terms of reports per 1000 doctors and reports per million population. New Zealand’s higher reporting rate is due to several factors: staff in the Centre for Adverse Reactions Monitoring are committed to providing feedback to individuals filing reports; outreach strategies, such as presentations on a monthly basis to health care providers are used to promote the Centre’s services and activities; education about ADR reporting is integrated into medical curricula; ADRs experienced by individuals are recorded with their National Health Index (NHI) number; previous ADRs are thus available to hospitals and increasingly general practitioners, through linkage with the NHI number, so that healthcare professionals are sensitized to look for future ADRs in these individuals.
Recommendations
• Health Canada needs to reorient its priorities so that postmarketing pharmacosurveillance is on an equal footing with approval of new drugs.
• Health Canada needs to devote significantly more resources to its postmarketing pharmacosurveillance system.
• Health Canada should undertake a systematic study to examine whether faster drug approvals lead to more postmarketing safety issues.
• Health Canada needs to develop measurable standards to judge its postmarketing pharmacosurveillance system.
• Health Canada needs to publicly and transparently explain what criteria it uses in issuing safety communications.
• Health Canada needs to systematically analyze whether its methods of communicating with health care professionals and the public are producing the desirable effects.
• Health Canada should adopt a form of the UK black triangle system to improve ADR reporting. One possibility is that a similar symbol could appear in the Compendium of Pharmaceuticals and Specialties and on all promotional material. In addition, it could be made mandatory for drug company sales representatives to inform doctors about drugs carrying this symbol that are made by their company.
• Health Canada should study the methods that New Zealand uses in its postmarketing ADR system and adapt them for Canadian use.
Joel Lexchin MSc, MD
Professor
School of Health Policy and Management
York University
and
Emergency Department
University Health Network
and
Associate Professor
Department of Family and Community Medicine
University of Toronto
Toronto, Ontario
Canada
Tel: 416-736-2100 x 22119
Fax: 416-736-5227
E mail: jlexchin@yorku.ca
joel.lexchin@utoronto.ca
References
1. Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies JAMA 1998; 279 (1200-1205).
2. Moore Thomas J., Cohen Michael R., Furberg Curt D. Serious Adverse Drug Events Reported to the Food and Drug Administration, 1998-2005. Archives of Internal Medicine 2007;167 1752-9.
3. Friedman MA, Woodcock J, Lumpkin MM, Shuren JE, Hass AE, Thompson LJ. The safety of newly approved medicines: do recent market removals mean there is a problem? JAMA 1999;281:1728-34.
4. Lexchin J. Relationship between pharmaceutical company user fees and drug approvals in Canada and Australia: a hypothesis-generating study. Annals of Pharmacotherapy 2006;40:2216-22.
5. Therapeutic Products Directorate. Business transformation progress report. Ottawa: Health Canada; 2004.
6. Government of Canada. The Canada we want: speech from the Throne to open the Second Session of the Thirty-Seventh Parliament of Canada. In; 2003.
7. External Advisory Committee on Smart Regulation. Risk management. nd. (Accessed at http://www.smartregulation.gc.ca/en/05/01/i4-01.asp. Accessed 2 February 2004.)
8. Health Canada. Health protection legislative renewal: detailed legislative proposal. Ottawa; 2003.
9. Department of Finance Canada. Building the Canada we want. Budget 2003: investing in Canada’s health care system [cat no F1-23/2003-4E]. Ottawa; 2003.
10. Health Canada. Improving Canada’s regulatory process for therapeutic products: building the action plan. Ottawa: Public Policy Forum multi-stakeholder consultation; 2003 November 2-3.
11. Abraham J, Davis C. A comparative analysis of drug safety withdrawals in the UK and the US (1971-1992): implications for current regulatory thinking and policy. Social Science and Medicine 2005;61:881-92.
12. Olson MK. Pharmaceutical policy change and the safety of new drugs. Journal of Law and Economics 2002;45:615-42.
13. Carpenter D, Bowers J, Grimmer J, Moffitt S, Nall C, Zucker EJ. Deadline effects in regulatory drug review: a methodological and empirical analysis; 2007.
14. Health Products and Food Branch. Cost recovery framework: official notice of fee proposal for human drugs and medical devices: Health Canada; 2007.
15. Health Products and Food Branch. Cost recovery framework: international comparison of fees and service standards for human drugs: Health Canada; 2007.
16. Graham DJ, Drinkard CR, Shatin D, Tsong Y, Burgess MJ. Liver enzyme monitoring in patients treated with troglitazone. JAMA 2001;286:831-3.
17. Willy ME, Manda B, Shatin D, Drinkard CR, Graham DJ. A study of compliance with FDA recommendations for pemoline (Cylert®). Journal of the American Academy of Child and Adolescent Psychiatry 2002;41:785-90.
18. Hazell L, Shakir SAW. Under reporting of adverse drug reactions: a systematic review. . Drug Safety 2006;29:385-96.
19. Moride Y, Haramburu F, Requejo A, Bégaud B. Under-reporting of adverse drug reactions in general practice. British Journal of Clinical Pharmacology 1997;43:177-81.
20. Decima Research Inc. Public opinion survey on key issues pertaining to post-market surveillance of marketed health products in Canada: final report. Ottawa: Health Canada; 2003 December. Report No.: POR# 298-02.
21. Hazell L, Shakir SAW. Under reporting of adverse drug reactions: a systematic review. Drug Safety 2006;29:385-96.
Page views since 15 March 2010: 5929
Comments
Our members can see and make comments on this page.













